Sam Bazrafshan, DPM*
Maria Pacheco, DPM*
Journal of the American Podiatric Medical Association Vol 107 – No 2 – March/April 2017
We report an unusual case of adenocarcinoma of the lung metastasizing to the proximal phalanx of the third digit in a 56-year-old woman with overlying complex regional pain syndrome. The patient was initially treated for neuroma, fracture, and neuropathic pain with no improvement over a 4-month period before presenting to the emergency department for left third digit pain. Radiographic imaging showed substantial osteopenia and mottling; magnetic resonance imaging demonstrated an aggressive lesion to the proximal phalanx. The patient underwent excision of the lesion, revealing metastatic moderately differentiated adenocarcinoma. (J Am Podiatric Med Assoc 107(2): 150-154, 2017) https://www.japmaonline.org/doi/abs/10.7547/15-179
Metastasis of primary tumors to the foot is uncommon; however, when it does occur, the most common sources are colorectal, kidney, and lung. Metastatic bone tumors greatly outnumber primary bone tumors. Based on the literature, metastasis to the hands and feet (acrometastases) occurs in only 0.007% to 0.3% of patients with malignancies. Statistics indicate a frequency of metastatic foot lesions of less than 2%.
Metastatic lesions of the foot are rarely reported, likely because of the difficulty or delay in diagnosis. Autopsy reports have documented that 20% to 70% of all patients who died of their malignant disease show microscopic evidence of osseous metastases. The first case of metastasis to the foot was reported in 1920 by Bloodgood.3 Metastatic tumors can occur in any bone in the foot. Lung carcinoma has been the most common malignancy reported to metastasize to the foot.
An increasing number of cases have been noted in the literature with findings of lung metastasis to the lower extremities. In 2002, a 71-year-old woman presented with atraumatic ankle pain, which resulted in a full radiographic work-up, revealing metastatic lung carcinoma to the distal fibula with bony erosion and pathologic fracture. Another such case involved metastasis of adenocarcinoma of the lung to the first metatarsal, initially diagnosed as gout. The patient underwent partial first-ray amputation and radiotherapy.
Although rare, adenocarcinoma metastasis to the phalanges of the foot has been reported. A similar case to the one encountered herein was a 67-year-old woman who presented with pain to the fifth digit, which resulted from metastasis of lung adenocarcinoma. The patient underwent excisional biopsy.7
Chronic regional pain syndrome (CRPS) is characterized by nonsegmental pain in one or more extremities combined with vasomotor instability, trophic changes, and radiographic osteopenia. It is now classified as two variants: CRPS I (reflex sympathetic dystrophy) is associated with a minor injury, fracture, or surgical procedure with no peripheral nerve injury, and CRPS II (otherwise known as causalgia) develops after damage to a peripheral nerve. Bone scans, particularly triphasic bone scans, add a higher degree of specificity for diagnostic purposes. However, CRPS is a clinical diagnosis and is sometimes considered a diagnosis of exclusion. In recent literature, the pathogenesis and mechanics have become better understood, but these are beyond the scope of this case report.
Reports of associations between CRPS and metastatic lesions are scattered throughout the literature. Various internal malignancies have been associated with CRPS since 1938, particularly the shoulder-hand variant. Two cases reported in 1984 of CRPS in the shoulder revealed an association with adenocarcinoma in the colon and axillary lymph node. Fewer cases have been reported in the lower extremity. A 2005 case of synovial sarcoma occurring in the knee of a 28-year-old woman was made 20 years after the onset of symptoms using magnetic resonance imaging (MRI) and needle biopsy. Findings from clinical examination and a triple-phase bone scan were consistent with a diagnosis of CRPS.
The purpose of this study was to contribute a case to the literature on the occurrence of metastasis of lung adenocarcinoma to the foot and its association, if any, with CRPS.
Case Report
A 56-year-old woman presented to the emergency department with pain in her left foot of 4 months’ duration after bumping her toe into a kitchen table. History revealed that the patient had initially sought treatment with several different physicians. She was treated for Morton’s neuroma and given corticosteroid injections, with no relief and exacerbation of her symptoms. She was referred to a neurologist, who sent her to undergo a nerve conduction study, which revealed no electrodiagnostic signs of peripheral nerve entrapment, although L5 radiculopathy was noted with electromyography. She was prescribed hydrocodone bitartrate and acetaminophen (Vicodin; AbbVie Inc, North Chicago, Illinois) and pregabalin (Lyrica; Pfizer Inc, New York, New York), again with little to no improvement, and was sent for physical therapy.
The patient returned to her primary care physician, who sent her for MRI of the foot, demonstrating a fracture of the left third proximal phalanx. She was referred to another foot and ankle specialist, who treated her with compression and immobilization in a pneumatic CAM Walker (Zinco Industries Inc, Pasadena, California). With her condition worsening she was further referred to a foot and ankle orthopedic surgeon, who evaluated her and diagnosed her as having neuritis and recommended injections for relief of her symptoms. The patient refused the injections and presented to the emergency department with pain to her left third toe and foot with symptoms of electrical shooting and pin-pricking pain to her left lower extremity. The patient also stated that she has a history of bronchitis over the past several months and a 30-year history of smoking tobacco.
On examination, the pedal pulses to the left foot were palpable, with all sensations to the limb intact. Diffuse erythema with a mottled appearance was noted on the skin dorsally, with moderate pitting edema of the left leg and foot. The skin of the left lower extremity was intact, with no acute clinical signs of infection. Pain with palpation was elicited from the third toe, as was pain with passive, but not active, range of motion. Radiographic evaluation revealed asymmetrical diffuse osteopenia compared with the contralateral side, with an irregular mottled appearance to the marrow of the distal foot with an aggressive erosive process involving the shaft of the third proximal phalanx. Findings from chest radiography were within normal limits, seemingly without signs of pulmonary involvement. A work-up was performed in the hospital, and the patient was referred to our services as an outpatient.
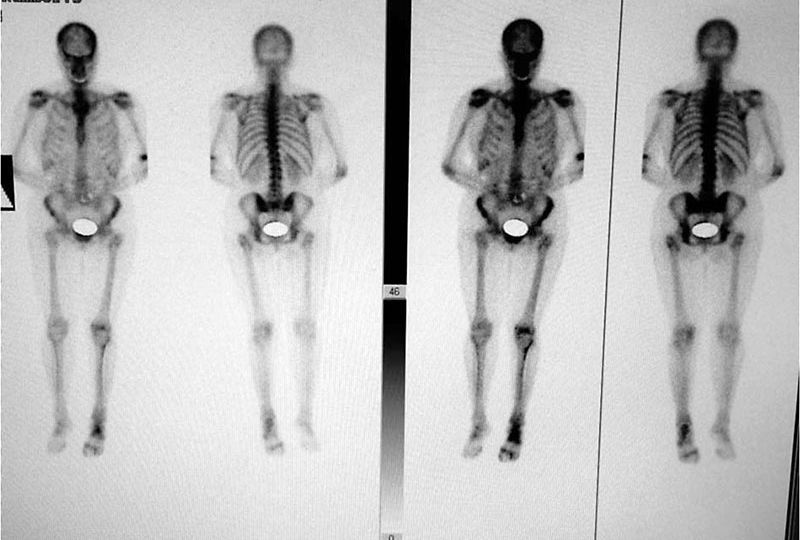
The patient was sent for a triple-phase bone scan and a second MRI to rule out a pathologic fracture and to help diagnose CRPS. The triple-phase bone scan revealed increased vascularity in the left foot centered at the third digit. Patchy areas of uptake were seen throughout the left lower extremity, specifically the left foot, with intense uptake. Radiograph showing diffuse osteopenia and cortical erosion of all of the bones but specifically of the third proximal phalanx.
Patchy areas of uptake were seen throughout the left lower extremity, specifically the left foot, with intense uptake to the third digit in the immediate delayed images. Abnormal delayed tracer uptake was diffusely seen in the tarsal bones, metatarsal bones, and phalanges, which was highly suggestive of CRPS.
An MRI was performed immediately, and its findings described an underlying aggressive process occurring in the left third toe. The left proximal phalanx of the third toe showed marrow signal abnormality with an expanded appearance and loss of cortical detail extending to the surrounding soft tissue. Owing to these findings, the patient was scheduled for a biopsy to definitively characterize the pathologic process.
The patient was taken to the operating room for bone and soft-tissue biopsy of the left third toe. A 3- cm incision was made to the dorsal aspect of the third toe from the proximal interphalangeal joint proximally to the third metatarsophalangeal joint. With careful dissection, it was immediately apparent that there was considerable disorganization of the soft-tissue structures and an atypical appearance of the anatomy. On encountering the proximal phalanx, the bone was noted to be soft and the cartilage was not adhered to the head of the proximal phalanx. A No. 15 blade was used to resect the head of the proximal phalanx due to lack of bony integrity. Bone, cartilage, and soft-tissue specimens were sent for cytologic and histopathologic analysis. The incision was then irrigated and closed in a standard manner.
Bone and tissue analysis revealed that the preliminary histopathologic findings were consistent with a metastatic moderately differentiated bronchogenic adenocarcinoma. An oncology consultation and a positron emission tomography scan were completed to identify the exact location of the primary tumor. Once the positron emission tomography findings were confirmed to be positive for metastasis from the lungs, the patient was referred to oncology for further medical management.
Under the direction of an oncologist, the patient began chemotherapy in an attempt to slow the progression of her metastases. However, the patient died several months into her chemotherapy treatment.
References
Discussion
A review of the literature noted few reports of lung adenocarcinoma metastasis to the foot. The diagnosis of solitary metastasis to the foot is difficult. Initial presentation usually includes nonspecific complaints of a painful and swollen foot. The present patient’s delay in diagnosis was likely due to the vague symptoms elicited by the tumor. Often, patients are first worked up and treated for more common conditions. Thus, it is not unusual for symptoms in the foot to become apparent before detection of the primary tumor. If possible, a detected tumor should be biopsied. Based on the results of histopathologic analysis in conjunction with advanced imaging, the site of the primary lesion can be determined. The treatment goals should also include reduction of symptoms and maintenance of weightbearing function to the involved extremity.
Occurrences of primary lesions metastasizing to the foot are uncommon in the literature, but the delay in diagnosis may have something to do with that as well. Hattrup et al reviewed cases of metastatic involvement in the foot and ankle, of which the most common primary tumor was lung carcinoma. He also found that diagnosis was delayed 1 to 24 months. Eggold et al reported a case of adenocarcinoma in the lung with phalangeal metastasis. In 2005, Ramkumar et al presented a case of adenocarcinoma in the distal phalanx of the hallux with the primary lesion located in the lung. Although the lesion was excised and biopsied, however unusual these cases may be, bone metastasis should be in the differential diagnosis. Leeson et al showed a 1.7% occurrence of metastasis to the feet in 827 autopsied patients with cancer and only 0.6% to the hand.
Infrequently, CRPS is associated with malignant circumstances. Complex regional pain syndrome is characterized by spontaneous pain disproportionate to the inciting injury, hyperalgesia, allodynia, sensorimotor dysfunction, edema, sudomotor abnormalities, and skin color changes. The diagnosis of CRPS is a diagnosis of exclusion. Therefore, the present case illustrates the importance of identifying a possible etiology for the CRPS due to it representing a systemic process that may be triggered by injury in another area of the body. Metastasis to bone is the most common cause of pain in patients with cancer, with many patients experiencing pain even before skeletal metastasis becomes radiographically apparent.
It can, therefore, be suggested that CRPS may represent a paraneoplastic syndrome in some cases. Ku et al14 suggested a causal relationship between their two cases of breast adenocarcinoma and lymphoma and the association with CRPS. However, as the mechanism of CRPS has become more recently understood, it is difficult to assess the relationship, if any, with malignancy.
It is speculation, in this case, whether the presence of CRPS was related to the ensuing metastatic adenocarcinoma or whether asymptomatic malignancy could have contributed to the pain biology and clinical presentation. It is difficult to deduce whether this patient developed CRPS as a result of the increasing aggression of the bone tumor to the area or whether this was a case of paraneoplastic syndrome, as suggested by other articles. The onset of CRPS without obvious injury or trauma may warrant a work-up for malignancy.