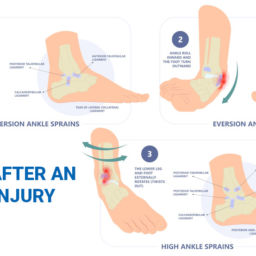
The inversion ankle sprain is the single most common injury in all of the sports and athletic injuries universally. If you regularly watch sporting events, you might see that an athlete is on injured reserve – this is likely due to an inversion ankle sprain. It makes up about 40% of all sports injuries, and 25% of all missed practice or play time. To further compound matters, the number one predisposing factor to suffer an ankle sprain is a history of a previous ankle sprain. This means that if you suffer one of these injuries you are exponentially more likely to get several others. However, what this also indicates is that if initial injuries are not rehabilitated and treated properly, you are more likely to have progressive deterioration and ankle instability to this very common and cumbersome injury.
Appropriate treatment of an ankle sprain injury involves a detailed history and physical examination – this is essentially to determine if ligaments are sprained or torn. Spraining basically implies overstretching of a ligament tissue and tearing means complete rupture and a possible detachment altogether. It also involves determining if there are any associated fractures or breakage of bones with the sprain. For example, it is possible to have any range of fractures including (a) an avulsion fracture of the base of the fifth metatarsal, (b) or a fracture of the anterior process of the calcaneus which is very common in this particular mechanism of a lateral ankle sprain.
Not to mention that repeated inversion ankle sprain injuries can put undue pressure within the joint itself and cause a compression or shearing injury on the surface of the cartilage – this is known as an osteochondral defect. If this is left untreated, it can eventually form what resembles a crater within the ankle joint.
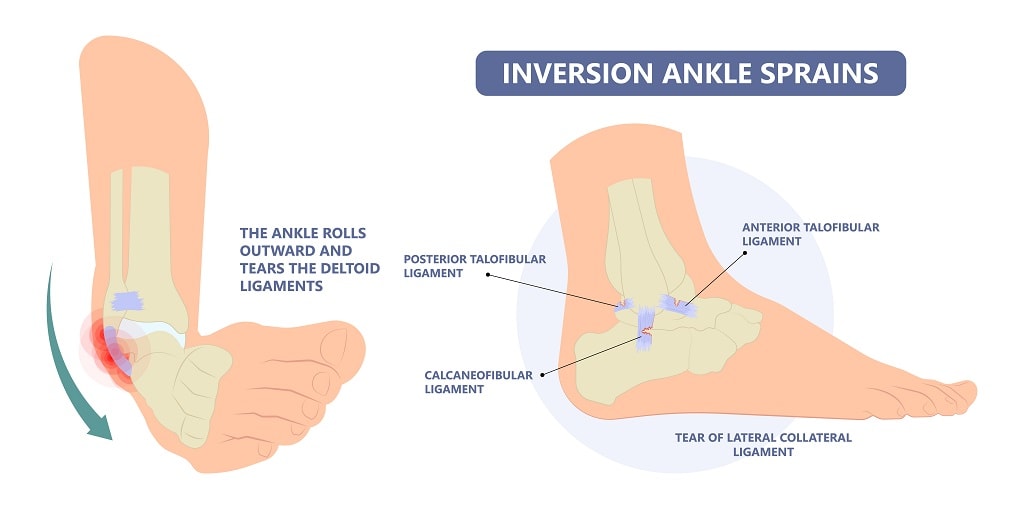
The three basic ligaments of the lateral ankle, which are anatomically more related to the sub talar joint:
- The anterior talofibular ligament (ATF)
- The calcaneo fibular ligament (CFL)
- The posterior talo fibular ligament (PTFL), which is also The most difficult ligament to sprain and injure.
There are 4 grades of ankle sprain injury based on the anatomy of the injured ligaments.
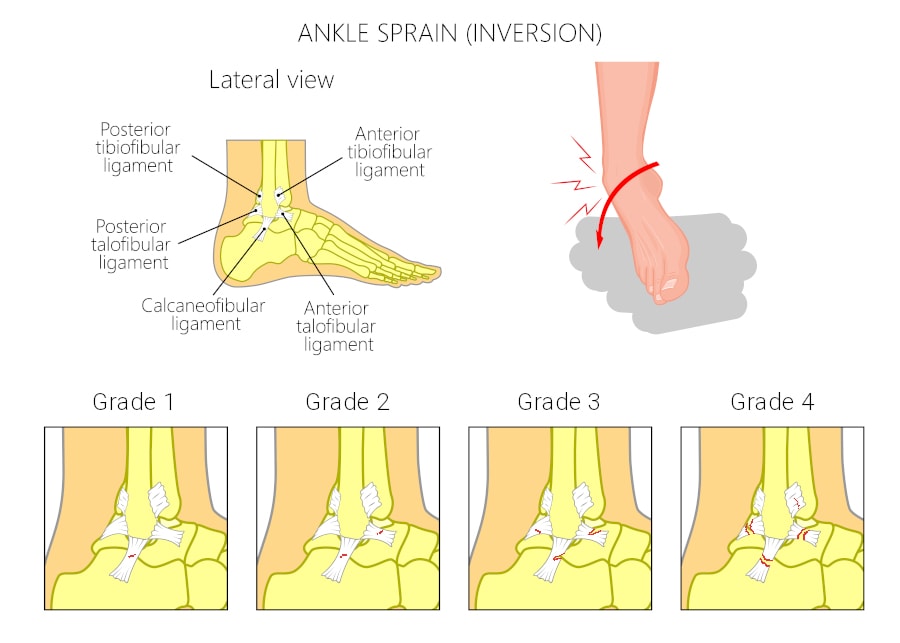
- Grade 1 – Is a sprain of ATF
- Grade 2 – Tear of ATF and sprain of CFL
- Grade 3 – Tear of ATF and CFL
- Grade 4 – Tear of ATF and CFL and sprain/tear of PTFL
The anterior talo fibular ligament is considered to be intracapsular and parts of the capsule that overlies the ankle and underlying subtalar joint. Integrity of this ligament is tested using a clinical maneuver known as the anterior drawer sign. This sign is considered positive if the talus is displaced forward 10 mm, or 4 mm more as compared with the contralateral side.
The talar tilt test is another clinical maneuver used to evaluate the integrity of the calcaneal fibular ligament, which is extracapsular and distinctive from the ankle capsule. If this maneuver is 5° or more as compared with the contralateral side, this is considered a positive finding. It correlates to abnormal stretching of the corresponding ligament being tested.
However, bear in mind that in individuals with functional injury, these clinical maneuvers may not necessarily be abnormal. This is because they are sensory receptors specifically affiliated with tendons, known as Golgi tendon organs that are very sensitive to both tension and pressure. They function like little nerves near and around the musculotendinous junctions. They help in regulation when a tendon has been overstretched and providing the corresponding reflex. When this system is normally functioning, they help to produce an inhibitory effect on the muscle/tendon unit that has been overstretched to prevent further injury to that tendon. However, as one might imagine in cases of chronic injury to the ligaments and tendons in the ankle and subtalar joints; the baseline of being overstretched is dysfunctional. So the damaged ankle is abnormally sprained in a way that the receptor feedback to the spinal cord produces a reflex that would normally cause a subconscious reflex in a person to avoid injury. In contrast, the person with chronic ankle instability cannot furnish the same protective reflex adequately or in time. This explains why once a person has had one ankle sprain, and if they are not properly rehabilitated they are likely to undergo these injuries over and over again.
Once an individual has initially protected, iced, compressed, elevated, and supported an injury, there are further options including: ankle bracing, taping, custom orthotics, nutritional supplements, shockwave therapy, amniotic fluid injections. The last resort is surgical reconstruction of the damaged tissue.
Crucial to reestablishing this neuromuscular feedback mechanism, is working together with physical therapy for proprioception and neuromuscular reeducation. This is done in an attempt to help to regain some of the somatosensory feedback mechanisms that were previously injured.
Talk to your certified podiatrist today to discuss which treatment options are best for you, so that you find the quickest and safest way possible to return to your athletic activity of choice.
by Dr. Felipe Peterson, DPM