Sarah Hubbard
*About the Author: Sarah Hubbard
Sarah Hubbard is a medical writer for Certified Foot and Ankle Specialists with approximately 15 years of experience creating accurate, patient-focused healthcare content. She specializes in translating complex podiatric topics into clear, informative articles that help patients better understand foot and ankle conditions, treatment options, and preventive care.
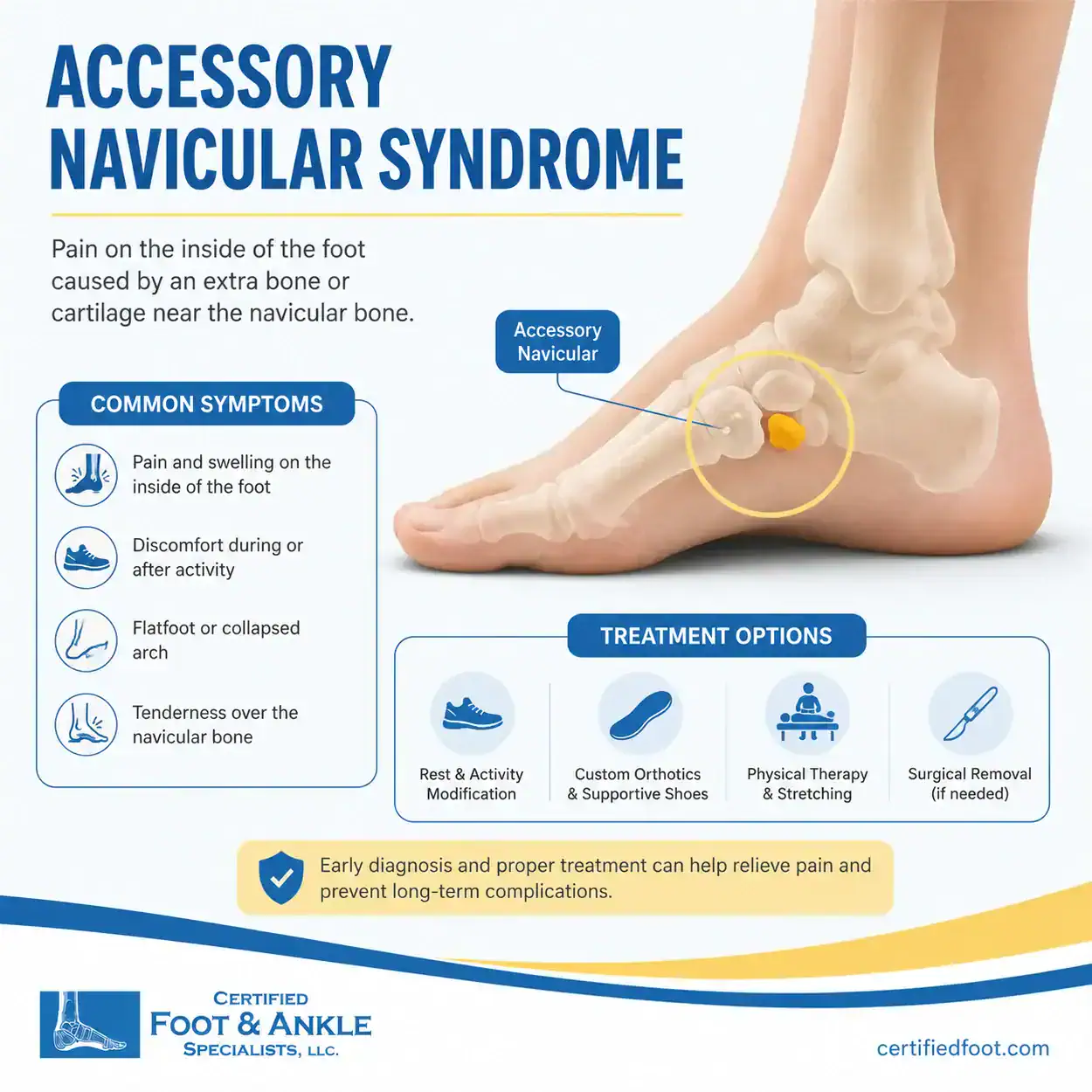
Accessory navicular syndrome is pain caused by an extra bone on the inner side of the foot near the navicular. A normal anatomical variant present in 10-15% of the population that becomes painful when the extra bone irritates the surrounding tendon or presses against footwear.
This extra bone, medically called the os tibiale externum, sits just above the arch of the foot. Most people who have one never experience any symptoms. But when it does cause pain, it can interfere with walking, sports, and wearing ordinary shoes — sometimes severely enough to affect daily life.
Quick Answers: Accessory Navicular Syndrome
What is accessory navicular syndrome? Pain from an extra bone (os tibiale externum) on the inner arch of the foot, present in 10-15% of people. It most commonly becomes symptomatic in adolescents and active adults when the extra bone stresses the posterior tibial tendon or rubs against footwear.
What causes it to become painful? Flat feet that overload the posterior tibial tendon, friction from narrow or rigid footwear, and repetitive physical activity. A foot or ankle sprain can also activate a previously silent accessory navicular.
How is it treated? Conservative care — orthotics, padding, activity modification, and a walking boot for flare-ups — resolves symptoms in 75-80% of patients within 6-12 weeks. Surgery (the Kidner procedure) is reserved for cases that don’t improve after 3-6 months of consistent conservative treatment.
How long is recovery from Kidner procedure surgery? Patients are typically non-weight-bearing for 6 weeks, return to daily activities at 8-10 weeks, and resume sports at 3-6 months post-operation.
Is accessory navicular bone dangerous? No. It’s a normal anatomical variant, not a disease or tumor. It doesn’t become cancerous, doesn’t spread, and doesn’t damage other bones. When it does cause pain, it responds well to conservative treatment in 75-80% of cases.
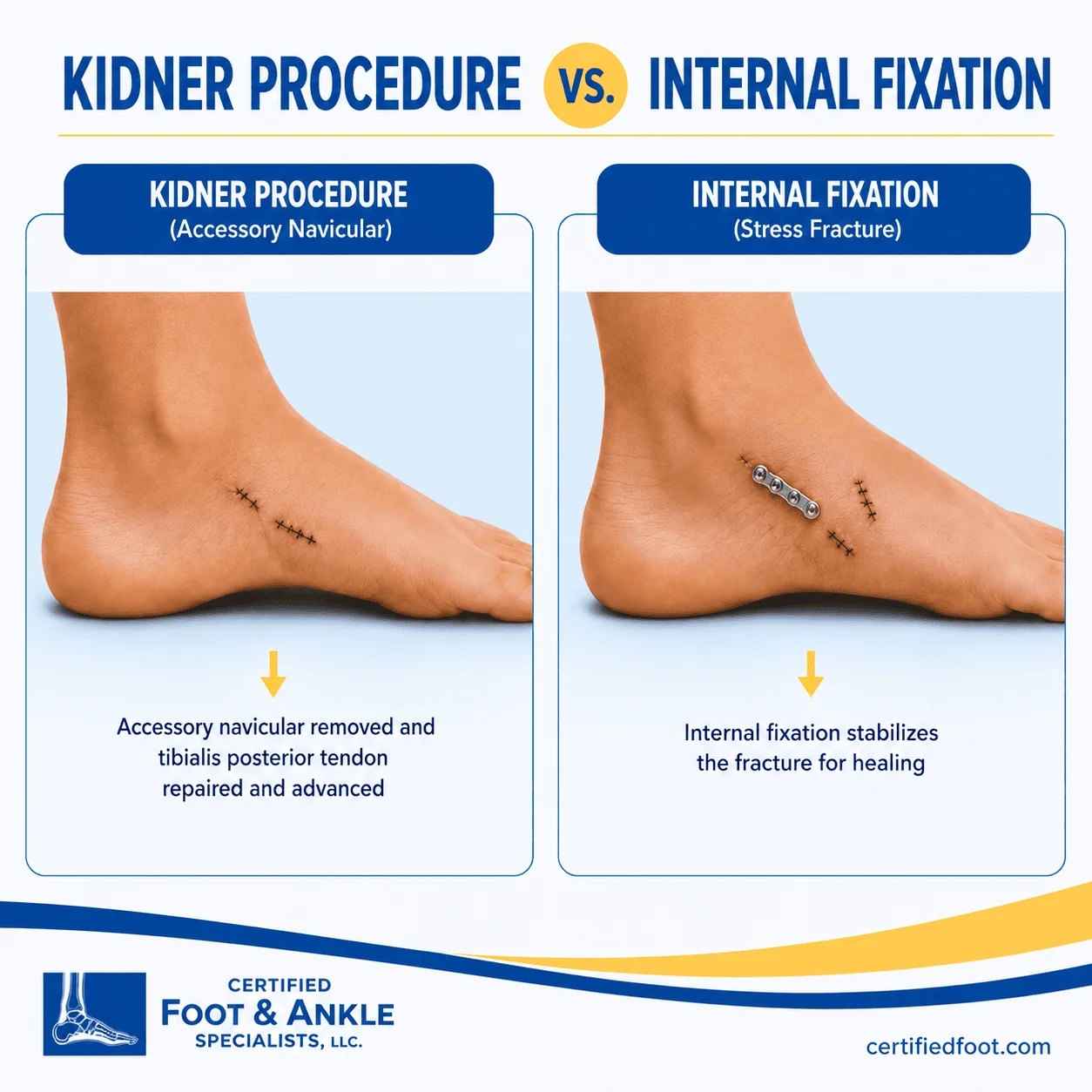
How is accessory navicular surgery different from navicular stress fracture surgery? The Kidner procedure removes an extra bone and reattaches a tendon — no screws cross the navicular. Stress fracture surgery uses 1-2 cannulated compression screws across the fracture line to promote healing. Same bone, completely different operations.
What is an accessory navicular bone?
An accessory navicular is an extra piece of bone that forms near the navicular during fetal development — a common anatomical variant, not an injury or disease. The navicular is the keystone bone of the medial arch of the foot, located between the ankle and the front of the arch. In some people, extra cartilage near that bone hardens into a separate bony fragment during adolescence rather than fusing with the navicular itself.
Certified Foot and Ankle Specialists is a multi-location podiatric surgery practice serving Southeast Florida and Southwest Florida, with board-certified foot and ankle surgeons treating accessory navicular syndrome. at locations across Fort Lauderdale, Coral Springs, Boca Raton, , Boynton Beach, West Palm Beach, Palm Harbor, Fort Myers, and Cape Coral.
What are the three types of accessory navicular?
Podiatrists classify accessory navicular bones using the Geist system, which organizes them by size, shape, and how they connect to the main navicular bone. Knowing your type determines which treatments are most likely to work.

Type 1 is a small, rounded ossicle
Roughly 2-3 mm embedded within the substance of the posterior tibial tendon. It’s the most common type and rarely causes symptoms because it’s fully enclosed within the tendon and doesn’t protrude enough to press against footwear.
Type 2 is a larger, triangular bone
Approximately 12 mm across that sits adjacent to the navicular and connects to it through a fibrocartilaginous bridge called a synchondrosis. Type 2 is the most commonly symptomatic form. The synchondrosis can become inflamed or develop micro-fractures under repetitive posterior tibial tendon loading — and this is what drives pain. Patients with Type 2 accessory navicular and flat feet are at the highest risk for developing symptoms.
Type 3 is a fused accessory bone
Essentially a Type 2 that merged with the navicular over time — creating a large, horn-shaped protrusion called a cornuate navicular. This produces a prominent bump on the inner foot that can cause significant friction against shoe counters.
What causes accessory navicular syndrome to become painful?
Having an accessory navicular doesn’t mean you’ll have pain. Symptoms develop only when the extra bone is stressed beyond its tolerance, and several specific factors drive that.
Flat feet (pes planus)
Is the biggest risk factor. When the medial arch collapses, the posterior tibial tendon is placed under greater load with every step because it works harder to support the arch. According to the American College of Foot and Ankle Surgeons (ACFAS), patients with flat feet and a Type 2 accessory navicular are significantly more likely to develop symptomatic disease than those with a normal arch. The flat-foot connection also explains why orthotics are so effective as a first-line treatment.
Physical activity
This accelerates the problem. Running, jumping, and lateral cutting sports like soccer, basketball, and tennis place repetitive strain on the synchondrosis. Adolescents are particularly vulnerable during growth spurts, when rapid skeletal changes increase bone stress at exactly the moment athletic participation is peaking.
Footwear causes direct irritation
Narrow toe boxes, rigid boot heel counters, and any shoe pressing against the medial navicular prominence can trigger skin inflammation, bursitis, and bone irritation.
A foot or ankle sprain can also activate a previously silent accessory navicular. The twisting force disrupts the synchondrosis, converting a pain-free anatomical variant into an actively symptomatic condition.
What are the symptoms of accessory navicular syndrome?
The most recognizable sign is a bony bump on the inner side of the foot between the arch and the ankle. Direct pressure on that prominence, even gentle pressing, typically hurts.
Beyond the bump, patients describe:
- Aching or throbbing pain along the inner arch, especially after standing or walking for more than 30-60 minutes
- Redness and warmth over the navicular prominence
- Localized swelling at the inner midfoot after activity
- Pain that worsens in narrow, stiff, or flat shoes
- In adolescents, a gradual limp that worsens across the school day or after practice
- In active adults, pain that prevents completing runs, hikes, or workouts at previous intensity
Symptoms typically improve with rest and worsen with activity. Constant pain even at rest is a red flag for a stress reaction or micro-fracture at the synchondrosis, and that warrants prompt evaluation.
Could this be a navicular stress fracture instead?
A navicular stress fracture is a crack in the main navicular bone itself. That makes it a completely different diagnosis from accessory navicular syndrome, which involves an extra bone sitting beside the navicular, not a fracture within it.
Both conditions cause midfoot pain. But the treatments are entirely different, so getting the diagnosis right matters.
The clearest difference is the bump. Accessory navicular syndrome produces a visible, firm lump on the inner foot you can press and immediately feel. A navicular stress fracture doesn’t do that. Pain spreads more broadly across the top or inner midfoot and builds up after repetitive impact activities like running, basketball, or military training. It’s not tied to a protrusion, and it’s not triggered by shoe friction.
Standard X-rays frequently miss navicular stress fractures. MRI or CT is required to confirm one, this is why a podiatric evaluation matters. The two conditions can look similar at first but need completely different treatment. Accessory navicular syndrome responds to orthotics or the Kidner procedure. A navicular stress fracture requires strict non-weight-bearing immobilization for 6–8 weeks, and displaced fractures need open reduction internal fixation (ORIF) surgery.
How do podiatrists treat accessory navicular syndrome?
Most cases resolve without surgery. Treatment starts with the least invasive options and escalates only when needed.
Conservative treatment
Donut padding is often the first and most immediately effective intervention. A horseshoe-shaped pad placed around the navicular prominence creates a pressure-free zone inside the shoe, reducing irritation while the area heals. It can be fitted during an office visit and provides relief the same day.
Custom orthotics address the underlying biomechanics that drive symptoms. They support the medial arch, control pronation, and reduce load on the posterior tibial tendon. A 2022 systematic review published in Current Reviews in Musculoskeletal Medicine found that orthotic therapy combined with activity modification produces meaningful symptom relief in 75-80% of patients who complete a full course of treatment.
Boot immobilization is used for acute flare-ups or when orthotics alone aren’t controlling symptoms. A CAM walker boot for 4-6 weeks offloads the synchondrosis completely and allows active inflammation to resolve. Over-the-counter NSAIDs (ibuprofen, naproxen) manage pain during this period.
Physical therapy follows immobilization. Targeted exercises for posterior tibial tendon strengthening, calf flexibility, and single-leg balance training reduce tendon load and help prevent recurrence once symptoms are under control.
Surgical treatment: the Kidner procedure
When 3-6 months of consistent conservative care don’t provide adequate relief, surgery is the appropriate next step. The Kidner procedure, first described in 1929, and is still the gold standard. This surgical procedure involves removing the accessory navicular bone, and advancing the posterior tibial tendon to a more mechanically favorable insertion point on the navicular. Thus improving its ability to support the arch.
The surgery takes approximately 45-60 minutes under regional or general anesthesia. It’s performed as an outpatient procedure; most patients go home the same day.
Recovery follows a predictable path. Patients are non-weight-bearing in a cast for 6 weeks, then transition to a walking boot for 2-4 additional weeks, then begin progressive rehabilitation. Return to sports typically takes 3-6 months. A 2022 systematic review in Current Reviews in Musculoskeletal Medicine reported that 80-90% of patients experience significant pain reduction and high satisfaction after the Kidner procedure.
For Type 1 or Type 3 presentations, where tendon advancement isn’t needed, a simpler excision of the extra bone is performed with a faster recovery.
Conservative treatment vs. Kidner procedure: decision guide
| Factor | Conservative Treatment | Kidner Procedure |
|---|---|---|
| Best for | First-time treatment; all Geist types | Failed conservative care (3-6 months); Type 2 |
| Downtime | 4-8 weeks (with orthotics) | 8-14 weeks total |
| Return to sports | 14-8 weeks (with orthotics) | 3-6 months |
| Hardware required | None | None — bone removed, tendon repositioned |
| Success Rate | 75-80% significant improvement | 80-90% report significant pain relief |
| When we use it | All newly diagnosed patients | After conservative care fails |
Does my teenager need treatment for accessory navicular syndrome?
Accessory navicular syndrome is most common in adolescents ages 10-14, when bone maturation coincides with peak athletic activity. Parents often notice a limp, a visible bump on the inner foot, or a child complaining that shoes hurt after school or after practice.
The reassuring reality: most adolescents with accessory navicular syndrome respond well to conservative care. Bones are still maturing in this age group, and symptoms often stabilize naturally by the late teens as skeletal growth completes and growth plates close.
Treatment in young patients follows the same conservative ladder as adults — padding, custom orthotics, activity modification, and boot immobilization for flare-ups. Surgery is rarely required in adolescents and is only considered when pain is consistently severe enough to limit daily activity or prevent sports participation despite 3-6 months of appropriate treatment.
If your child has a bump on the inside of the foot and is walking differently, avoiding gym class, or dropping out of sports they used to enjoy, a podiatric evaluation is the right first step. Early fitting of custom orthotics frequently prevents symptom progression and eliminates the need for any surgical discussion.
How is accessory navicular surgery different from navicular stress fracture surgery?
The navicular is involved in both conditions, but these are completely different problems requiring completely different operations. Patients who’ve been told they need “navicular surgery” should know exactly which procedure is being discussed — and why.
Accessory navicular surgery (Kidner procedure) treats a bone that was always there — an extra bone you were born with. The goal is to remove it and reattach the posterior tibial tendon to where it should be. No screws cross the navicular bone itself. No bone graft is needed. It’s a soft tissue reconstruction combined with bone removal, and hardware is typically limited to a small anchor for the tendon reattachment.
Navicular stress fracture surgery treats a bone that has cracked under repetitive loading stress. The goal is compression of the fracture line to restore bone continuity and promote healing. This is done with 1-2 cannulated compression screws placed across the fracture under fluoroscopic guidance. A bone graft may be added for delayed union or poor blood supply cases. The hardware typically stays in permanently unless it becomes symptomatic.
Kidner procedure vs. navicular stress fracture surgery: side by side
| Factor | Kidner Procedure (Accessory Navicular) | Internal Fixation (Stress Fracture) |
|---|---|---|
| Problem treated | Extra bone irritating posterior tibial tendon | Crack in navicular from repetitive impact loading |
| Goal of surgery | Remove extra bone; reattach posterior tibial tendon | Compress fracture line; restore bone continuity |
| Hardware used | Tendon anchor; no screws across navicular bone | 1-2 cannulated compression screws across fracture line |
| Bone graft needed | No | Sometimes — for non-union or poor blood supply |
| Incision | Small medial incision over navicular | Percutaneous (minimal) or open dorsal for displaced fractures |
| Hardware permanent | N/A — no crossing hardware | Usually permanent; removed only if symptomatic |
| Weight bearing post-op | Non-weight-bearing 6-8 weeks | Non-weight-bearing 6 weeks; longer if displaced |
| Full recovery | 3-6 months | 3-6 months; up to 9 months for return to sport |
| Typical patient | Adults with flat feet and chronic inner arch pain | Runners, track athletes, military recruits |
If you’ve been diagnosed with a navicular stress fracture rather than accessory navicular syndrome, the treatment pathway is different. Navicular stress fractures are managed first with strict non-weight-bearing immobilization, with surgical screw fixation reserved for complete or displaced fractures. See our guide to foot fracture surgery and open reduction internal fixation (ORIF) for a full explanation of how these injuries are classified and when fixation is required.
When should you see a podiatrist for foot arch pain?
Not every bump near the arch requires urgent care. But certain signs mean it’s time to get a proper diagnosis.
See a podiatrist if:
- A visible or palpable bump has appeared on the inner side of your foot or your child’s foot
- Arch pain has persisted for more than 2-4 weeks despite rest and over-the-counter anti-inflammatories
- Pain is severe enough to cause a limp or limit participation in sports, work, or daily activities
- The bump is red, warm, or showing skin breakdown from shoe friction
- A recent ankle sprain triggered new inner foot pain that hasn’t resolved in 1-2 weeks
- A teenager is withdrawing from sports or activities due to foot pain
At Certified Foot and Ankle Specialists, evaluation begins with weight-bearing X-rays to classify the accessory navicular type and assess arch structure. If symptoms are severe or surgery is being considered, an MRI can confirm synchondrosis edema, posterior tibial tendon integrity, and any associated flat-foot changes before a treatment decision is made.
The bottom line
Accessory navicular syndrome is painful, but it responds well to treatment. Most patients — teens and adults alike — achieve lasting relief through orthotics, activity modification, and a short period of immobilization. Surgery is effective when conservative care falls short, with 80-90% of patients reporting significant improvement after the Kidner procedure.
If arch pain is limiting your daily routine or your child’s sports participation, Dr. Ashley Bowles, DPM, FACFAS, CWSP, at Certified Foot and Ankle Specialists can evaluate whether an accessory navicular is the source and build a treatment plan that fits your life. On Florida’s West Coast, Dr. Victor L. Herrera, DPM, ABMSP, sees patients in the Fort Myers area. Contact us to schedule a consultation, or find a location nearest to you.